
Abstract and Introduction
Abstract
This article is one of ten reviews selected from the Annual Update in Intensive Care and Emergency Medicine 2023. Other selected articles can be found online at https://www.biomedcentral.com/collections/annualupdate2023. Further information about the Annual Update in Intensive Care and Emergency Medicine is available from https://link.springer.com/bookseries/8901.
Introduction
Patients admitted to the intensive care unit (ICU) with acute respiratory failure frequently fulfil the criteria for acute respiratory distress syndrome (ARDS).[1] The diagnosis is based on radiological, physiological, and clinical criteria described in the 'Berlin definition' (Table 1).[2] Yet establishing the diagnosis of ARDS has limited treatment consequences in and of itself, as the available evidence-based interventions are mainly related to minimizing iatrogenic damage (e.g., ventilator-induced lung injury [VILI] and fluid overload) rather than the use of specific treat-ments. Whereas the intervention options for the syndrome itself are limited, adequate and timely treatment of the causal underlying condition has a major impact on the improvement of outcomes for patients with ARDS.[3]
The classical description of ARDS relies on the histological finding of diffuse alveolar damage secondary to another condition (one of the clinical risk factors described in Table 1).[4] Diffuse alveolar damage is an untreatable finding and must be distinguished from a large number of diseases that also meet the ARDS syndrome definition but are treatable.[5] Table 2 provides an overview of the differential diagnoses that must be taken into account in patients suspected of having ARDS.
It should be possible to establish a definitive causal diagnosis within 7 days after onset in the vast majority of patients with ARDS. Yet, the often chaotic nature of clinical reality can lead to a delayed and haphazard search for underlying causes, especially in patients with multiple important problems.
This narrative review aims to provide a structured approach to the diagnosis of underlying conditions in patients who fulfil the ARDS criteria according to the Berlin definition, in order to enable underlying causes to be rapidly and adequately treated. The diagnostic steps are described point by point in three phases and are summarized in a flowchart (Figure 1). We also provide a summary of the most important uncertainties relevant to clinicians managing patients with ARDS.
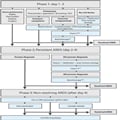
Figure 1.
Flowchart for diagnostic steps in patient with ARDS. *Including exposure to drugs, animals, toxic fumes, vaping. **Chest computed tomography (CT) with high resolution (HR) images, preferably with an inspiratory hold. ***Send for tests described under point 6 in phase 1 in the text. qPCR quantitative polymerase chain reaction, CMV cytomegalovirus, BAL bronchoalveo- lar lavage, ILD interstitial lung disease
With the steps and timeframe described here, we have intended to strike a balance between early and vigorous diagnostic investigations where needed and a more parsimonious approach where appropriate. Nevertheless, the authors' experience is one rooted in academic medicine in a resource-rich environment. The details of our approach should therefore be adapted to local resources and possibilities. The most important aspect of the here described approach is not the number of laboratory investigations or imaging modalities, but rather the structuredness and timeliness of the diagnostic evaluation.
Crit Care. 2023;27(94) © 2023 BioMed Central, Ltd.
Copyright to this article is held by the author(s), licensee BioMed Central Ltd. This is an Open Access article: verbatim copying and redistribution of this article are permitted in all media for any purpose, provided this notice is preserved along with the article's original citation.













