This article originally appeared on Hospital for Special Surgery's website.
Case Report
An 81-year-old man with a left shoulder hemiarthroplasty performed 12 years prior fell while gardening and sustained a left periprosthetic humeral shaft fracture. His medical history included coronary artery disease treated with cardiac stents, hyperlipidemia, hypertension, and colon cancer in remission after chemotherapy and resection.
He presented 10 days after injury and was neurovascularly intact. His left shoulder had relatively poor range of motion prior to the injury, but the patient lived independently and performed all activities of daily living. Radiographs demonstrated a transverse fracture through the cement mantle of a well-fixed cemented left shoulder hemiarthroplasty (Figure 1). He was indicated for open reduction and internal fixation of the left humerus.
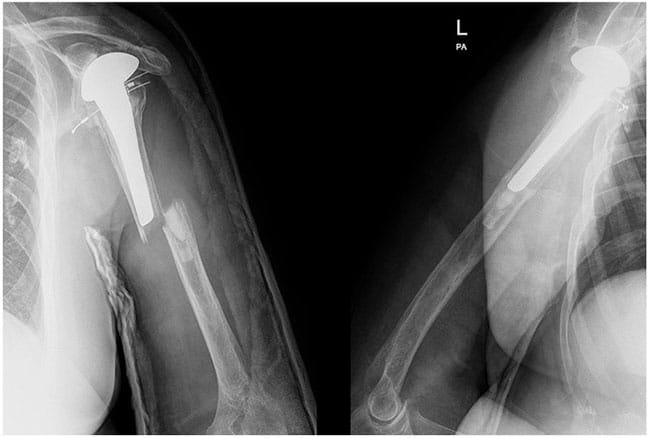
Figure 1. Anteroposterior and lateral images at presentation show a transverse fracture through a cemented left shoulder hemiarthroplasty performed 12 years prior.
Preoperative planning for this patient revealed difficulties commonly seen with periprosthetic humerus fractures. Standard humeral plates would allow only for unicortical screw placement in the proximal fragment due to the patient's arthroplasty stem. Unicortical screws offer inadequate rotational control, and so a periprosthetic plate with offset screw holes was selected in order to increase the likelihood of gaining adequate proximal fixation. As a backup, cerclage cables were available and a posterior approach was utilized to visualize the radial nerve and facilitate safe cable passage around the humerus if needed.
Intraoperatively, a posterior triceps splitting approach was used and the radial nerve was dissected and protected. The humeral stem was confirmed to be well fixed within the cement mantle. Next, the transverse fracture was reduced using clamps placed inside drill holes and the clamps replaced with a medial mini-fragment plate to hold the reduction. A periprosthetic plate used posteriorly allowed for placement of multiple bicortical and transcortical screws around the implant stem (Figure 2). The plate was fixed distally in standard fashion with bicortical nonlocking and locking screws.
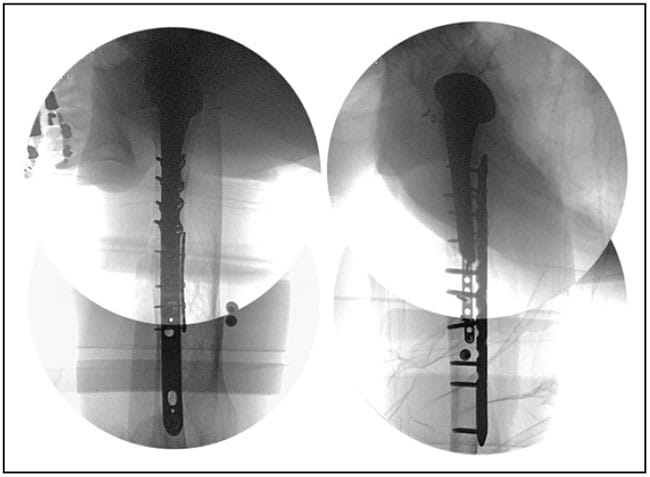
Figure 2. Intraoperative fluoroscopy shows a dual-plate construct using mini- and large-fragment plates.
After surgery, the patient was neurovascularly intact. Physical therapy included coffee-cup weightbearing with pendulum exercises for the shoulder and active and passive range of motion of the elbow, forearm, wrist, and hand. At 6 weeks postoperatively, radiographs revealed callus formation with no evidence of hardware failure (Figure 3). The patient progressed to be weightbearing as tolerated and began active and passive range of motion of the shoulder. At final follow-up, he was able to live and function independently.

Figure 3. Radiographs at 6 weeks after surgery show callus formation.
Discussion
Postoperative periprosthetic humeral fractures with shoulder arthroplasties using a stem have a higher rate of nonunion due to preferential force transmission through the fracture site, as well as disruption to the endosteal blood supply.[1] Indications for surgical management remain controversial, and studies examining these injuries have small sample sizes and a focus on anatomic total shoulder replacements with standard-length stems.[2,3,4,5,6,7,8] Fractures proximal to or near the tip of the stem are more likely to require surgery because of increased strain due to implant stiffness and risk for implant loosening.[9] Fractures that are well distal to the tip of the stem are more amenable to nonoperative management, as these mimic non-periprosthetic fractures more closely.[10] In a series of 16 periprosthetic humerus fractures treated with surgery, nine patients were dissatisfied mostly due to loss of shoulder motion; the average time between fracture fixation and union was 278 days.[4]
In this patient, we utilized several techniques to overcome the difficulties often faced with this fracture type. A mini-fragment plate was used to hold the reduction for provisional maintenance while a definitive implant was applied, a technique that is useful for many different fracture types.[11] Next, we used a definitive plate with offset screw holes for the placement of bicortical or transcortical fixation around the humeral stem. Unicortical screws are significantly weaker in torsion than bicortical screws, and torsional forces are commonly encountered in the humeral shaft.
This technique also obviates the use of cables, which are inferior biomechanically and pose a risk to the surrounding neurovascular structures during placement.[12]
Credits:
Images: Hospital for Special Surgery
Grand Rounds From HSS: Management of Complex Cases © 2023 Hospital for Special Surgery
Cite this: Aleksey Dvorzhinskiy, William M. Ricci. Obtaining Adequate Fixation in a Periprosthetic Humerus Fracture Around a Shoulder Arthroplasty Stem in 81-Year-Old Man - Medscape - Apr 17, 2023.









Comments